
The only practice in Western Massachusetts exclusively dedicated to the care of the hand and upper extremity.
Saturday, November 4, 2017
Turkey Carving Safety Tips
Every year, people severely cut their hand while carving a turkey. Luckily, these injuries are avoidable. Common sense knife technique combined with well establish Turkey carving tips will help to avoid problems.
If you cut your finger or hand, bleeding from minor cuts will often stop by applying direct pressure to the wound with a clean cloth.
Wednesday, June 21, 2017
Fireworks Safety 4th of July and beyond
With the Fourth of July holiday fast approaching, experts are urging people to use caution when handling fireworks and have provided a list of safety tips to consider.
According to the latest U.S. Consumer Product Safety Commission report, fireworks sent roughly 11,000 people to the emergency room over the course of the Fourth of July holiday. Of these injuries, approximately 36 percent were to the hand, thumb and digits. Interesting enough, 40% of the injuries are caused by fireworks that were thought to be somewhat safe such as sparklers and firecrackers.
The number of firework-related injuries treated in emergency rooms in the United States has ranged from 8,500 to 9,800 since 1997; in 2011, 26% of patients were younger than age 15.1 Firework-related injuries range in severity from superficial burns to complete loss of the hand and fingers. The most common injuries are burns to the fingers, hand, and wrist (26.7%), followed by injuries to the eye (14.9%), and open injuries to the hand and wrist (6.5%).2 Other sources report that the number of burns to the fingers, hand, and arm are as high as 41%.3 Burns account for more than 50% of firework-related injuries,
Recent years were especially injurious and many high profile injuries occurred. Such as to the NFL's Jason Pierre Paul and in 2015 fireworks injuries reached a 15 year high.
Be responsible when incorporating fireworks into your holiday and summer festivities. Provided below are 10 fireworks safety tips to keep yourself and others safe:
- While lighting fireworks, never position any part of your body over them
- After lighting fireworks, immediately back up to a safe distance
- To avoid burns from sparklers, poke a hole at the bottom of a cup and put the handle of the sparkler through the hole. This technique will shield your hand from sparks that are emitted from the sparkler. It’s also important to wear gloves when using sparklers (leather preferred) as they can be as hot as a blow torch and over 15 times hotter than boiling water.
- Never attempt to re-light or handle malfunctioning fireworks
- Light only one firework at a time – at arm’s length – with an extended lighter
- Always wear eye protection/safety glasses when lighting fireworks
- Never carry a firework in your pocket or shoot them from a metal or glass container
- Never aim or throw fireworks at another person, animal or building
- Have a bucket of water or working garden hose accessible
- Properly dispose of all fireworks (used and unused). Allow used fireworks to soak in water for a few hours before discarding.
The following precautions should be taken when attending a public fireworks display:
- Obey safety barriers and ushers.
- Stay back a minimum of 500 feet from the launching site.
- Resist the temptation to pick up firework debris when the display is over. The debris may still be hot, or in some cases, the debris might be “live” and could still explode.
- Ensure all children have adult supervision.
The potential long-term severity of fireworks-related injuries can have undesirable outcomes to the body, so remember to enjoy the holiday safely and responsibly and don’t take any unnecessary risks.
1. Hall JR Jr. Fireworks. Quincy, MA: National Fire Protection Association; 2013.
2. Canner JK, Haider AH, Selvarajah S, et al. US emergency department visits for fireworks injuries, 2006-2010. J Surg Res. 2014;190(1):305e311.
3. Fireworks information center: United States Consumer Product Safety Commission Website. http://www.cpsc.gov/PageFiles/150398/Fireworks-Infographic-2015-web.pdf?epslanguage=en Published 2013. Accessed June 29, 2015.
3. Fireworks information center: United States Consumer Product Safety Commission Website. http://www.cpsc.gov/PageFiles/150398/Fireworks-Infographic-2015-web.pdf?epslanguage=en Published 2013. Accessed June 29, 2015.
portions taken from assh.org and other sources such as
Monday, March 6, 2017

Wednesday, February 8, 2017
WINTER STORM SNOWBLOWER ALERT...AGAIN
As physicians dedicated to the care of the Hand and Upper extremity we want to inform the public concerning the perils and pitfalls of improper snow blower use. Physicians, nurses, allied health professionals and therapists who deal with these injuries live in fear of the first heavy wet snow of the season. Invariably injuries are seen despite general knowledge that these injuries occur. These safety tips cannot guarantee against injury but hopefully if you are reading these or even better spreading these, it is one more step towards preventing these types of injuries.
Recommendations for safe use of a jammed snow blower snow blowers include: (OCD STICK)
1. If the snow blower jams, immediately turn it OFF
2. Disengage the CLUTCH
3. DELAY...Wait 10 seconds after shutting of to allow Impeller Blades to stop rotating
4. Always use a STICK or broom handle to clear impacted snow. The stick most be strong enough to avoid breakage or eye injures can result from flying fragments.
5. Never put your hand near chute or around blades
6. Keep all shields in place. Do not remove safety devices on machine
7. Keep hands and feet away from moving parts
8. Keep a clear head, concentrate and ...
Do not drink alcoholic beverages before using a snow blower
Keep Fingers and Hands Safe: Practice Snowblower Safety
Each year hundreds of people suffer maiming or amputations of their fingers or hands due to the improper handling of snowblowers
The American Society for Surgery of the Hand would like to provide you with patient information to help you avoid these injuries during the winter season.
Injury Profile
Average age: 44 years
Sex: Male
Dominant hand — 90% of injuries
Amputations of tips of fingers
Middle finger most commonly injured
Average age: 44 years
Sex: Male
Dominant hand — 90% of injuries
Amputations of tips of fingers
Middle finger most commonly injured
Common Weather Conditions
- Heavy, wet snow
- Large snow accumulation, greater than six inches
- Temperature: 28 degrees Fahrenheit or greater
Injury Causes
- Snow clogging the exit chute of the machine
- Not noticing that the impeller blades are still rotating even though the machine is off
- Operator attempts to clean the clogged exit chute with hands
- Hands connect with the rotating blades, resulting in severe injury
Snowblowers are safe if used properly.
more information:
Monday, January 9, 2017
WINTER ADVISORY FROSTBITE of the FINGERS PREVENT FROSTBITE
WINTER ADVISORY FROSTBITE of the FINGERS PREVENT FROSTBITE
FROSTBITE
Frostbite occurs when the skin is overexposed to extreme cold. It can occur when the temperature and/or wind chill is below 27°F (-3°C), and it typically occurs in the fingers and toes.Cases of frostbite are “typically the result of overexposure —skiers, snowboarders and climbers who don't have the luxury of warming up in the lodge because they have ventured off the grid.” But it can occur anywhere that the temperature and windchill puts fingers or toes at risk
SYMPTOMS AND TREATMENT
When caught early, most frostbite is superficial and therefore reversible. If your fingertips are white, numb and swollen, see your doctor as soon as possible. Do not rewarm your fingers if you will be overexposing them to cold weather again. Your doctor will take care of rewarming the affected areas, and a hand surgeon may be brought in to take care of any blisters.
FROSTBITE IN CHILDREN
If you are with a young child who is complaining of being cold, then go inside. once frostbite sets in, the child will stop complaining because the area becomes numb and he or she cannot feel the problem. It is important to monitor children and yourself for signs of frostbite.
PREVENTION
To prevent frostbite, limit your time outside during cold weather; if you must venture outside, wear appropriate clothing. In extremely cold temperatures, winter athletes should consider electric boot warmers to protect their toes or gloves and mittens that have electric warming systems to protect their fingers, especially if they sustained frostbite in the past. Winter sports participants should heed warnings posted by the mountain on very cold days.
SOURCE includes information edited and taken from ASSH Frostbite post
PREVENT FROSTBITE As windchill increases time to frostbite decreases

https://www.assh.org/handcare/About-Hand-Surgery/Media/Details/ArticleID/45492/Frostbite-in-the-Hand READ ABOUT...
Posted by The Hand Center of Western Massachusetts on Friday, January 9, 2016
Friday, September 30, 2016
Dr. Martin leaves hand surgery
Dr. Martin no longer be sees patients at the Hand Center of Western
Massachusetts. If you are a
patient of the Hand Center, we would like to assure you that your will continue to receive the utmost level of
care and attention to detail that you have come to expect.
Our plan is to offer
continuity of care for all patients at the Hand Center.
Dr. Wint and Dr. Wintman
are available to answer questions regarding your current treatment or to schedule new or
follow-up appointments. We will continue to be on call for the office and
its patients. When you call after hours, no matter what the situation is, you
will get one of them to answer your questions.
Our office
structure is something that we have developed over many years and we feel it is
our attention to detail that allows us to offer care at the highest
level. In addition we are always looking for ways to improve so please
let us know how we can better help you
in the future.
If you have any
questions please do not hesitate to contact the office.
Monday, August 22, 2016
SCAPHOID FRACTURES OF THE WRIST
SCAPHOID FRACTURES of the WRIST
Scaphoid Fractures
What are scaphoid fractures?
The scaphoid bone is one of the eight small bones that make up the “carpal bones” of the wrist. There are two rows of bones, one closer to the forearm (proximal row) and the other closer to the hand (distal row). The scaphoid bone is unique in that it links the two rows together (see Figure 1). This puts it at extra risk for injury, which accounts for it being the most commonly fractured carpal bone.
How do scaphoid fractures occur?
Fractures of the scaphoid occur most commonly from a fall on the outstretched hand. Usually it hurts at first, but the pain may improve quickly, over the course of days or weeks. Bruising is rare, and there is usually no visible deformity and only minimal swelling. Since there is no deformity, many people with this injury mistakenly assume that they have just sprained their wrist, leading to a delay in seeking evaluation. It is common for people who have fractured this bone to not become aware of it until months or years after the event.
Diagnosis of scaphoid fractures
Scaphoid fractures are most commonly diagnosed by x-rays of the wrist. However, when the fracture is not displaced, x-rays taken early (first week) may appear negative. A non-displaced scaphoid fracture could thus be incorrectly diagnosed as a “sprain.” Therefore a patient who has significant tenderness directly over the scaphoid bone (which is located in the hollow at the thumb side of the wrist, or “snuffbox”) should be suspected of having a scaphoid fracture and be splinted (see Figure 2). An X-ray a couple of weeks later may then more clearly reveal the fracture. In questionable cases, MRI scan, CT scan, or bone scan may be used to help diagnose an acute scaphoid fracture. CT scan and/or MRI are also used to assess fracture displacement and configuration. Until a definitive diagnosis is made, the patient should remain splinted to prevent movement of a possible fracture.
Treatment of scaphoid fractures
If the fracture is non-displaced, it can be treated by immobilization in a cast that usually covers the forearm, hand, and thumb, and sometimes includes the elbow for the first phase of immobilization. Healing time in a cast can range from 6- 10 weeks and even longer. This is because the blood supply to the bone is variable and can be disrupted by the fracture, impairing bony healing. Part of the bone might even die after fracture due to loss of its blood supply, particularly in the proximal third of the bone, the part closest to the forearm. If the fracture is in this zone, or if it is at all displaced, surgery is more likely to be recommended. With surgery, a screw or pins are inserted to stabilize the fracture, sometimes with a bone graft to help heal the bone (see Figure 3a,3b). Surgery to place a screw may also be recommended in non-displaced cases to avoid prolonged casting.
Complications of scaphoid fractures
Non-union: If a scaphoid fracture goes unrecognized, it often will not heal. Sometimes, even with treatment, it may not heal because of poor blood supply(seeFigure 3c). Over time, the abnormal motion and collapse of the bone fragments may lead to mal-alignment within the wrist and subsequent arthritis. If caught before arthritis has developed, surgery may be performed to try to get the scaphoid to heal.
Avascular necrosis: A portion of the scaphoid may die because of lack of blood supply, leading to collapse of the bone and later arthritis. Fractures in the proximal one third of the bone, the part closest to the forearm, are more vulnerable to this complication. Again, if arthritis has not developed, surgery to try to stabilize the fracture and restore circulation to the bone may be attempted. (see.Figure 4)
Post-traumatic arthritis: If arthritis has already developed, salvage-type procedures may be considered, such as removal of degenerated bone or partial or complete fusion of the wrist joint.
Figure 1: The scaphoid bone is unique in that it spans the two rows of wrist bones making it more prone to injury from a fall in full extension

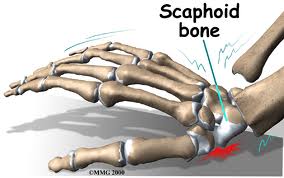

Figure 2: Significant tenderness directly over the scaphoid bone (which is located in the hollow at the thumb side of the wrist).
Figure 3a,3b: A screw or pins are placed to stabilize the fracture.


Figure 3c. The scaphoid has a variable pattern of blood supply that may predispose it to AVN and delayed healing

Figure 4. An MRI may be used to diagnose Avascular Necrosis (AVN) after a scaphoid fracture has not healed

parts © 2011 American Society for Surgery of the Hand. Developed by the ASSH Public Education Committee and Modified and supplemented for this blog by www.handcttr.com
Subscribe to:
Posts (Atom)