Wrist Sprains and Ligament Injuries
What is a sprain?
A sprain is an injury to a ligament. Ligaments are the connective tissues that connect and stabilize one bone to another bone; they could be thought of as very strong tape that holds the bones together at a joint (see Figure 1). The degree of ligament injury may vary over a wide range of severity. Sprains are generally classified into three types: Grade I – stable injury to a ligament; Grade II – partial tearing/stretching; and Grade III – complete tear of the ligament, either within the mid-portion of the ligament, or as an avulsion (“pulling away”) from its attachment into bone. A sprain may upset the normal coordinated movements of the wrist bones resulting in persistent stiffness, pain, swelling, and possible instability.
How do wrist sprains occur?A sprain of one or multiple wrist ligaments occurs when there is excessive loading or force transmitted across the wrist. These frequently occur as the result of a fall forwards or backwards onto an outstretched hand. Force may be applied in other ways, such as with a violent twisting injury (torsion). Often, these injuries are associated with sports and other outdoor activities such as biking, skiing, or snowboarding.
What are the most common types of wrist sprains?
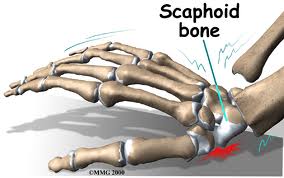
There are many ligaments which stabilize the wrist joint. One of the most common ligament injuries involves the scapho-lunate ligament, the ligament which links the scaphoid and lunate bones (Figure 2).
Another wrist ligament injury that often occurs is the Lunato-triquetral ligament which connects two bones in the wrist called the lunate and the triquetrum.
Scapho-Lunate ligament injury
is the most common and most significant ligament injury of wrist;
Many risk factors for this injury such as ulna minus configuation, slope of radial articular surface, and lunotriquetral coalition;
As in all wrist ligament injuries there is a range of injury from that of a mild teat to that of increasing severity such as
dynamic scapholunate instability Some would call this spectrum a range from a intrinsic intraosseous ligament microtear vs a large full scale tear and associated extrinsic ligament injury. While x-rays may not show any initial radiographic evidence of malalignment is present a diagnosis is established by dorsal S-L tenderness and positive shift test; late finding may include rotatory subluxationand later dynamic or static changes to the alignment of the carpal bones
Lunatotriqetral injury or LT ligament injury
is often associated with Lunotriquetral Dissociation or ulnar side carpal instability;A sprain is an injury to a ligament. Ligaments are the connective tissues that connect and stabilize one bone to another bone; they could be thought of as very strong tape that holds the bones together at a joint (see Figure 1). The degree of ligament injury may vary over a wide range of severity. Sprains are generally classified into three types: Grade I – stable injury to a ligament; Grade II – partial tearing/stretching; and Grade III – complete tear of the ligament, either within the mid-portion of the ligament, or as an avulsion (“pulling away”) from its attachment into bone. A sprain may upset the normal coordinated movements of the wrist bones resulting in persistent stiffness, pain, swelling, and possible instability.
How do wrist sprains occur?A sprain of one or multiple wrist ligaments occurs when there is excessive loading or force transmitted across the wrist. These frequently occur as the result of a fall forwards or backwards onto an outstretched hand. Force may be applied in other ways, such as with a violent twisting injury (torsion). Often, these injuries are associated with sports and other outdoor activities such as biking, skiing, or snowboarding.
What are the most common types of wrist sprains?
There are many ligaments which stabilize the wrist joint. One of the most common ligament injuries involves the scapho-lunate ligament, the ligament which links the scaphoid and lunate bones (Figure 2).
Another wrist ligament injury that often occurs is the Lunato-triquetral ligament which connects two bones in the wrist called the lunate and the triquetrum.
Scapho-Lunate ligament injury
is the most common and most significant ligament injury of wrist;
Many risk factors for this injury such as ulna minus configuation, slope of radial articular surface, and lunotriquetral coalition;
As in all wrist ligament injuries there is a range of injury from that of a mild teat to that of increasing severity such as
dynamic scapholunate instability Some would call this spectrum a range from a intrinsic intraosseous ligament microtear vs a large full scale tear and associated extrinsic ligament injury. While x-rays may not show any initial radiographic evidence of malalignment is present a diagnosis is established by dorsal S-L tenderness and positive shift test; late finding may include rotatory subluxationand later dynamic or static changes to the alignment of the carpal bones
Lunatotriqetral injury or LT ligament injury
that involves disruption of lunotriquetral & volar radiolunotriquetral ligaments and attentuation or rupture of dorsal radiotriquetral attachments. There are several different degrees of injury.
A grade one injury involves a isolated tear of the LT interosseous ligament and there will be only a small amount of increased motion, however, even this is enough to cause symptoms; A grade three injury represents a complete disruptionand there can be malrotationof the bones if a high grade or grade three injury is left untreated. The mechanism of the injury occurs with forced extension or extension and simultaneous radial deviation, as scaphoid induces the lunate into a further flexion stance while triquetrum extends;
As mentioned with a grade three or advanced injury, lunotriquetral, volar radiolunotriequetral, and dorsal radiotriquetral ligaments are torn and malrotation or a VISI collapse deformity develops either acutely or over time.
How are wrist sprains diagnosed?The diagnosis of a wrist sprain includes a careful patient history (how the injury occurred), a clinical examination, and diagnostic testing. The patient typically presents with complaints of wrist pain and stiffness, and loss of strength is also common. Examination of the wrist will allow your hand surgeon to pinpoint tenderness and thus localize the site of injury, and also assess wrist stability. Usually X-rays are obtained to evaluate for potential fractures and for signs of ligament insufficiency. While ligaments themselves are not seen on X-rays, the consequence of a ligament injury may be appreciated indirectly based on abnormal alignment of the wrist bones (Figure 3). Additional diagnostic testing may be required, such as an MRI or an MRI-arthrogram, which involves an injection of contrast into the wrist to enhance the sensitivity of the MRI. Wrist arthroscopy is a very precise, direct way to examine the wrist ligaments. It is a surgical procedure in which a small scope and specialized instruments are placed into various parts of the wrist joint via several small (approximately 3mm) incisions. However, the risks and benefits of the surgery must be considered relative to the severity of the wrist injury.
How are wrist sprains treated?The goals of treating a wrist ligament injury are to:
- provide pain relief
- minimize potential stiffness or loss of motion
- restore wrist joint stability
- reduce the risk of long-term consequences of an untreated wrist ligament injury (arthritis, pain, instability)
The treatment of a wrist sprain is guided by the severity of the injury. Similar to a sprained ankle, milder ligament sprains of the wrist may be treated with protected activity, supportive splinting or casting, strategies to minimize inflammation and discomfort, and gradual return to activity. Evaluation by a hand surgeon will help grade the severity of the injury, identify associated injuries, and determine the need for more specific diagnostic testing.
For less severe wrist sprains, the ligaments usually heal well – occasionally, the injury and healing response may cause stiffness and your hand surgeon may recommend stretching and motion exercises to minimize the potential for longer term loss of wrist mobility.
In the case of a ligament tear, treatment may or may not involve surgery; treatment depends on the specific ligament injury and individual patient needs and considerations. For certain injuries, wrist arthroscopy may be recommended to evaluate the wrist and to possibly trim loose or inflamed flaps from the injured ligament. If the findings are more severe, your surgeon may need to proceed with an open ligament repair or reconstruction. The ligaments themselves are not always very substantial, and so repairs may need to be augmented with additional tissue such as the joint capsule or various tendon grafts, especially if the injury is not being treated acutely. There is much research underway searching for better methods to treat these serious injuries. They include stronger and more precise ligament reconstructions using either local tissues (tendons) or distant tissues (ligaments from the hand or foot). Pins or screws are often used to help stabilize the repairs as well. Your surgeon will discuss the various options based on the specifics of your injury.
Treatment of Lunate Triquetrum ligament tears
Arthroscopy allows the best method of determining whether LT instability is present;
In severe or chronic cases lunotriquetral arthrodesis may be indicated for disabling pain after non operative treatment measures have failed. Most patients may expect good to excellent relief of pain, up to 80% of normal wrist motion and upto 90% maintenance of grip strength
Chronic wrist sprains
Unrecognized or untreated ligament injuries may result in wrist instability which leads to progressive cartilage degeneration (arthritis) in the wrist joint. This arthritic change may result in pain, stiffness, and swelling; these symptoms may be intermittent and vary in their severity. A common pattern is seen with scapho-lunate ligament tears that alter the normal wrist joint mechanics. The unlinked scaphoid rotates away from the lunate. As a result of the abnormal rotation of the scaphoid, its joint surface no longer makes contact with the radius bone properly. Instead of broad contact along the entire joint surface, there is “edge on edge” contact of the joint, wearing it down in a predictable progressive pattern of arthritis. This form of arthritis is known as scapho-lunate advanced collapse, or “SLAC” wrist, which progresses to involve a greater amount of the wrist over time, thereby limiting treatment options. A good analogy is that of placing two spoons into a drawer; normally they are placed flush with one another, with the greatest surface area of contact. However, if the spoons are rotated slightly, they match up “edge on edge” and no longer have a good, broad surface area where they touch each other.
In the presence of a chronic wrist ligament injury and associated arthritis, mild / intermittent symptoms may be treated with splinting, activity modifications, and analgesics, such as anti-inflammatory medications. Persistent symptoms or a symptom flare may be treated with a steroid injection.
Should these conservative measures fail, surgery may be considered in order to remove the offending, arthritic joint surfaces, such as with a proximal row carpectomy (remove the arthritic first row of wrist bones, which includes the scaphoid), or scaphoidectomy and partial wrist fusion (remove the arthritic scaphoid bone and fuse four small wrist bones together for stability). In the case of more widespread wrist arthritis, wrist arthroplasty (joint replacement) or total wrist fusion may be performed.

Figure 1: Ligaments of wrist

Figure 2: Diagram of the scapholunate ligament (circled)


Figure 3: X-ray showing gap between scaphoid and lunate from ligament rupture (right) and normal x-ray of opposite wrist (left)
parts© 2006 American Society for Surgery of the Hand but modified and appended by www.handctr.com
How are wrist sprains treated?The goals of treating a wrist ligament injury are to:
- provide pain relief
- minimize potential stiffness or loss of motion
- restore wrist joint stability
- reduce the risk of long-term consequences of an untreated wrist ligament injury (arthritis, pain, instability)
The treatment of a wrist sprain is guided by the severity of the injury. Similar to a sprained ankle, milder ligament sprains of the wrist may be treated with protected activity, supportive splinting or casting, strategies to minimize inflammation and discomfort, and gradual return to activity. Evaluation by a hand surgeon will help grade the severity of the injury, identify associated injuries, and determine the need for more specific diagnostic testing.
For less severe wrist sprains, the ligaments usually heal well – occasionally, the injury and healing response may cause stiffness and your hand surgeon may recommend stretching and motion exercises to minimize the potential for longer term loss of wrist mobility.
In the case of a ligament tear, treatment may or may not involve surgery; treatment depends on the specific ligament injury and individual patient needs and considerations. For certain injuries, wrist arthroscopy may be recommended to evaluate the wrist and to possibly trim loose or inflamed flaps from the injured ligament. If the findings are more severe, your surgeon may need to proceed with an open ligament repair or reconstruction. The ligaments themselves are not always very substantial, and so repairs may need to be augmented with additional tissue such as the joint capsule or various tendon grafts, especially if the injury is not being treated acutely. There is much research underway searching for better methods to treat these serious injuries. They include stronger and more precise ligament reconstructions using either local tissues (tendons) or distant tissues (ligaments from the hand or foot). Pins or screws are often used to help stabilize the repairs as well. Your surgeon will discuss the various options based on the specifics of your injury.
Treatment of Lunate Triquetrum ligament tears
Arthroscopy allows the best method of determining whether LT instability is present;
In severe or chronic cases lunotriquetral arthrodesis may be indicated for disabling pain after non operative treatment measures have failed. Most patients may expect good to excellent relief of pain, up to 80% of normal wrist motion and upto 90% maintenance of grip strength
Chronic wrist sprains
Unrecognized or untreated ligament injuries may result in wrist instability which leads to progressive cartilage degeneration (arthritis) in the wrist joint. This arthritic change may result in pain, stiffness, and swelling; these symptoms may be intermittent and vary in their severity. A common pattern is seen with scapho-lunate ligament tears that alter the normal wrist joint mechanics. The unlinked scaphoid rotates away from the lunate. As a result of the abnormal rotation of the scaphoid, its joint surface no longer makes contact with the radius bone properly. Instead of broad contact along the entire joint surface, there is “edge on edge” contact of the joint, wearing it down in a predictable progressive pattern of arthritis. This form of arthritis is known as scapho-lunate advanced collapse, or “SLAC” wrist, which progresses to involve a greater amount of the wrist over time, thereby limiting treatment options. A good analogy is that of placing two spoons into a drawer; normally they are placed flush with one another, with the greatest surface area of contact. However, if the spoons are rotated slightly, they match up “edge on edge” and no longer have a good, broad surface area where they touch each other.
In the presence of a chronic wrist ligament injury and associated arthritis, mild / intermittent symptoms may be treated with splinting, activity modifications, and analgesics, such as anti-inflammatory medications. Persistent symptoms or a symptom flare may be treated with a steroid injection.
Should these conservative measures fail, surgery may be considered in order to remove the offending, arthritic joint surfaces, such as with a proximal row carpectomy (remove the arthritic first row of wrist bones, which includes the scaphoid), or scaphoidectomy and partial wrist fusion (remove the arthritic scaphoid bone and fuse four small wrist bones together for stability). In the case of more widespread wrist arthritis, wrist arthroplasty (joint replacement) or total wrist fusion may be performed.
Figure 1: Ligaments of wrist
Figure 2: Diagram of the scapholunate ligament (circled)
Figure 3: X-ray showing gap between scaphoid and lunate from ligament rupture (right) and normal x-ray of opposite wrist (left)
parts© 2006 American Society for Surgery of the Hand but modified and appended by www.handctr.com
REFERENCES