What are scaphoid fractures?
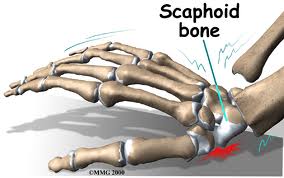
The scaphoid bone is one of the eight small bones that make up the “carpal bones” of the wrist. There are two rows of bones, one closer to the forearm (proximal row) and the other closer to
the hand (distal row). The scaphoid bone is unique in that it links the two rows together (see Figure 1). This puts it at extra risk for injury, which accounts for it being the most commonly fractured carpal bone.
How do scaphoid fractures occur?
Fractures of the scaphoid occur most commonly from a fall on the outstretched hand.
Usually it hurts at first, but the pain may improve quickly, over the course of days or weeks.
Bruising is rare, and there is usually no visible deformity and only minimal swelling.
Since there is no deformity, many people with this injury mistakenly assume that
they have just sprained their wrist, leading to a delay in seeking evaluation.
It is common for people who have fractured this bone to not become aware
of it until months or years after the event.
Diagnosis of scaphoid fractures
Scaphoid fractures are most commonly diagnosed by x-rays of the wrist. However,
when the fracture is not displaced, x-rays taken early (first week) may appear negative.
A non-displaced scaphoid fracture could thus be incorrectly diagnosed as a “sprain.”
Therefore a patient who has significant tenderness directly over the scaphoid bone
(which is located in the hollow at the thumb side of the wrist, or “snuffbox”)
should be suspected of having a scaphoid fracture and be splinted (see Figure 2).
An X-ray a couple of weeks later may then more clearly reveal the fracture.
In questionable cases, MRI scan, CT scan, or bone scan may be used to help
diagnose an acute scaphoid fracture. CT scan and/or MRI are also used to
assess fracture displacement and configuration. Until a definitive diagnosis
is made, the patient should remain splinted to prevent movement of a
possible fracture.
Treatment of scaphoid fractures
If the fracture is non-displaced, it can be treated by immobilization in a cast
that usually covers the forearm, hand, and thumb, and sometimes includes
the elbow for the first phase of immobilization. Healing time in a cast can
range from 6- 10 weeks and even longer. This is because the blood supply
to the bone is variable and can be disrupted by the fracture, impairing bony
healing. Part of the bone might even die after fracture due to loss of its
blood supply, particularly in the proximal third of the bone, the part closest
to the forearm. If the fracture is in this zone, or if it is at all displaced,
surgery is more likely to be recommended. With surgery, a screw or pins
are inserted to stabilize the fracture, sometimes with a bone graft to help
heal the bone (see Figure 3a,3b). Surgery to place a screw may also be
recommended in non-displaced cases to avoid prolonged casting.
Complications of scaphoid fractures
Non-union: If a scaphoid fracture goes unrecognized, it often will not heal.
Sometimes, even with treatment, it may not heal because of poor blood
supply(seeFigure 3c). Over time, the abnormal motion and collapse of the
bone fragments may lead to mal-alignment within the wrist and subsequent
arthritis. If caught before arthritis has developed, surgery may be performed to
try to get the scaphoid to heal.
Avascular necrosis: A portion of the scaphoid may die because of lack of blood supply, leading to collapse of the bone and later arthritis. Fractures in the proximal one third of the bone, the part closest to the forearm, are more vulnerable to this complication. Again, if arthritis has not developed, surgery to try to stabilize the fracture and restore circulation to the bone may be attempted. (see.Figure 4)
Post-traumatic arthritis: If arthritis has already developed, salvage-type procedures may be considered, such as removal of degenerated bone or partial or complete fusion of the wrist joint.
Figure 1: The scaphoid bone is unique in that it spans the two rows of wrist bones making it more prone to injury from a fall in full extension
Figure 2: Significant tenderness directly over the scaphoid bone (which is located in the hollow at the thumb side of the wrist).
Figure 3a,3b: A screw or pins are placed to stabilize the fracture.
Figure 3c. The scaphoid has a varialbe pattern of blood supply that may predispose it to AVN and delayed healing
Figure 4. An MRI may be used to diagnose Avascular Necrosis (AVN) after a scaphoid fracture has not healed
parts © 2011 American Society for Surgery of the Hand. Developed by the ASSH Public Education Committee and Modified and supplemented for this blog by www.handcttr.com